Are Implants Forever? Surprising Truths and Current Evidence on Treating Peri‑Implantitis
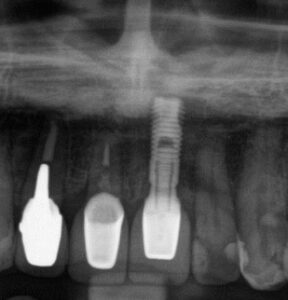
Director doctor placed this Swedish implant names Astra Implant 15 years ago. It still works.
Are Implants Forever? Surprising Truths and Current Evidence on Treating Peri‑Implantitis
Introduction — the hidden pitfall of the “second permanent tooth”
Dental implants are now a mainstream solution for missing teeth, often hailed as a “second permanent tooth.” That expectation — that implants require no maintenance and will last a lifetime — is common but misleading. Implants are inert devices surrounded by living tissues and are vulnerable to bacterial plaque–driven inflammation, i.e., peri‑implant mucositis and peri‑implantitis. If inflammation progresses, the supporting tissues can be destroyed and the implant may ultimately fail. Implants are not a “set‑and‑forget” cure; they are a delicate device that requires lifelong management.
Experience (clinical perspective)
In clinical practice I have seen many implant cases and the consequences when maintenance and inflammation control are insufficient. The scientific literature and systematic reviews show unexpected findings that should inform how clinicians and patients approach implant care and peri‑implantitis treatment.
Expertise (evidence summary)
A recent Cochrane review synthesizing 15 studies (9 meeting strict criteria) evaluated surgical and non‑surgical interventions for peri‑implantitis. Contrary to intuitive expectations, the analysis did not find clear evidence that complex, costly surgical approaches outperform basic subgingival mechanical debridement in clinically meaningful ways. In short: advanced surgery has not been proven superior to careful mechanical cleaning below the gumline.
Key findings and interpretation
- Complex, expensive treatment is not proven superior
The review found no consistent evidence from several trials that more complex, surgical approaches provided greater benefit than conventional subgingival mechanical debridement. The fundamental reason is biological: successful control of peri‑implantitis depends first and foremost on controlling the local bacterial environment. No current surgical technique has demonstrated overwhelming additional value beyond effective bacterial removal and maintenance. - Recurrence is common — peri‑implantitis behaves like a chronic disease
Peri‑implantitis is often chronic and relapsing. Some studies with follow‑up >1 year reported very high recurrence rates — in some treatment arms approaching 100%. This underscores that peri‑implantitis rarely resolves permanently after a single intervention; ongoing control and maintenance are essential. Maintenance is not optional — it is an integral component of treatment success. - Small signals of benefit (but limited and preliminary)
A few trials showed modest, statistically significant improvements with adjunctive measures in specific contexts:
- Local antibiotics: In severe cases with >50% bone loss, adding local antibiotics to mechanical debridement produced small additional improvements in probing pocket depth (PPD ≈ 0.59 mm) and clinical attachment (PAL ≈ 0.61 mm) at 4 months.
- Xenograft bone substitute (Bio‑Oss) + resorbable membrane: In defects ≥3 mm, use of xenograft and barrier showed greater PPD and PAL gains (≈1.4 mm) at 4‑year follow‑up compared with synthetic graft in one small trial.
These differences are measured in millimeters and, while potentially meaningful at the microscopic level, come from small, biased or uncertain trials and thus remain provisional.
- What the evidence does — and does not — tell us
Current evidence does not indicate that any single treatment protocol is clearly the best. That does not mean interventions are meaningless; rather, high‑quality, long‑term randomized trials are lacking to establish superiority among approaches. The field needs larger, well‑designed studies with ≥1‑year follow‑up to define optimal strategies.
Clinical implications — practical guidance for patients and clinicians
- Prevention and inflammation control are paramount. Because evidence for a definitive “best” treatment is lacking, the most reliable strategy is rigorous prevention and lifelong maintenance: plaque control, patient self‑care, smoking cessation, and regular professional recall.
- When peri‑implantitis occurs, individualized treatment planning is required. Consider defect morphology, severity, patient systemic risk factors, and the patient’s ability to maintain hygiene. Adjuncts such as local antibiotics or grafting materials may offer incremental benefit in selected cases but should be considered provisional.
- Realistic expectations: inform patients that peri‑implantitis is often chronic, may recur, and requires sustained effort rather than a single curative procedure.
Conclusion — a candid perspective
We do not yet have a definitive “best” treatment for peri‑implantitis. Given the current evidence, the most important measures are prevention, strict bacterial control, and persistent maintenance. If you are considering implants — or already have them — prioritize daily self‑care and regular professional maintenance over the assumption that a complex procedure alone will secure lifelong success. Your best defense for the “second permanent tooth” is consistent care and vigilance, not one‑time, high‑cost interventions
Reference
Esposito, M., Grusovin, M. G., & Worthington, H. V. (2012). Interventions for replacing missing teeth: treatment of peri‐implantitis. Cochrane database of systematic reviews, (1).
Make an appointment for consultation today.
Tokyo International Dental Clinic Roppongi
- Address: 5-13-25-2nd Floor, Roppongi, Minato-ku, Tokyo
- Phone: 03-5544-8544
- Closest Stations:
- Azabu Juban (Toei Oedo Line take exit7)
- https://youtu.be/iIeG91YEJTA The way to the clinic from Ohedo Line Exit7
- Azabu Juban (Tokyo Metro Namboku Line exit 5a )
- https://youtu.be/3yniFSfucGg The way to the clinic from Namboku Line Exit 5a
- Roppongi (Hibiya Line exit 3)
We look forward to helping you achieve a healthy, beautiful smile!