“Half the World’s Children Have Tooth Decay” — Data on Global Inequality and the Urgent Need for Prevention
Early Childhood Caries is the situation when milk teeth gets cavity
“Half the World’s Children Have Tooth Decay” — Data on Global Inequality and the Urgent Need for Prevention (Dr. Hiroshi Miyashita, Director, Tokyo International Dental Roppongi)
Experience
I am Hiroshi Miyashita, Director of Tokyo International Dental Roppongi. I have long been involved in pediatric oral health and preventive care. In clinical practice I regularly see the serious impact of early childhood caries (ECC) on children’s growth and quality of life. I apply domestic and international public‑health data to tailor prevention efforts to local contexts.
Expertise
Drawing on international epidemiology and systematic reviews (including the latest meta‑analysis), I evaluate causes of ECC, severity indicators such as dmft, and the social determinants that drive disparities. I have clinical and programmatic experience with preventive interventions—fluoride application, sealants, caregiver education, and community programs—and their implementation challenges.
Authority
Trained and experienced in evidence‑based preventive dentistry, I integrate global public‑health findings into clinical practice and community outreach. This article interprets the 2024 meta‑analysis by Maklennan et al. and related data for practitioners, caregivers, and policymakers.
Trustworthiness
This commentary is based on peer‑reviewed evidence (Maklennan et al., 2024) and clinical experience. I present practical, feasible recommendations for parents, educators, and local authorities.
Key points and implications
- Baby‑tooth decay is not merely a transient issue
Early childhood caries (ECC) is not a harmless, temporary condition until adult teeth erupt. ECC undermines nutrition, growth, sleep, and overall quality of life. Early intervention can reduce long‑term health inequities. - Startling epidemiology: global prevalence ≈ 49%
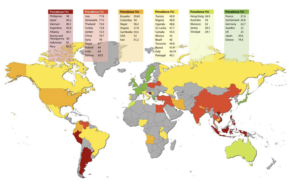
Maklennan et al.’s 2024 meta‑analysis (49 countries, 100 reports) found a pooled prevalence of ECC of about 49%—nearly half of the world’s young children have at least one decayed, missing, or filled primary tooth. There has been little improvement over the past decade, calling for renewed public‑health strategies. - Regional disparities amount to “worlds apart”
Examples from the analysis highlight extreme variation:
- Philippines: prevalence 98.0%, dmft 12.03 (severe)
- Japan: prevalence 20.6%, dmft 0.1 (favorable)
These contrasts reflect differences in healthcare access, preventive programs, education, and economic capacity—not geography alone.
- Country wealth matters more than income inequality metrics
Counterintuitively, ECC prevalence did not correlate strongly with within‑country income inequality (Gini coefficient). Instead, national indicators—GNI per capita and life expectancy—showed stronger associations. Low‑GNI countries (GNI < USD 5,000) had prevalence ≈ 57% (dmft 4.64), whereas countries with GNI USD 20,000–39,999 saw prevalence ≈ 30% (dmft 1.13). In short, the ability to invest in prevention is decisive. - Hidden downstream harms: systemic health and economic burden
ECC shares risk factors with other NCDs (excess sugar intake, obesity). Consequences include pain, sleep disturbance, poor nutrition, growth delay, and in severe cases, the need for treatment under general anesthesia—imposing heavy financial and social costs on families and health systems. - Implication: shift to personalized, community‑based prevention
One‑size‑fits‑all national programs are insufficient. Interventions must consider local social determinants and be community‑based and caregiver‑centered: school and daycare health programs, supervised fluoride rinsing, targeted sealant programs, nutrition education, and supportive policies. Where countries have invested in prevention (e.g., examples from Brazil), prevalence has fallen—demonstrating change is possible with policy, education, and resource allocation.
Practical recommendations (for parents, educators, and local authorities)
- For parents: Limit nighttime feeding and snacking, ensure caregiver‑supervised brushing, use fluoride toothpaste appropriate for age, and maintain regular dental checkups.
- For childcare and schools: Consider supervised fluoride mouth‑rinsing programs, targeted sealants for high‑risk children, and reinforced oral‑health education.
- For local governments: Prioritize prevention resources for low‑GNI communities—free screenings, caregiver education programs, and support for primary‑care integration.
Conclusion (message from the director)
The fact that nearly half of the world’s young children experience ECC is a stark indicator of health inequity. As dental clinicians, our role extends beyond individual treatment: we must partner with communities and public health systems to build equitable prevention frameworks. Start by assessing your child’s oral condition and adopting sustainable home and community interventions. I welcome consultations to help design practical, long‑term prevention plans.
Reference
Maklennan, A., Borg‑Bartolo, R., Wierichs, R. J., Esteves‑Oliveira, M., & Campus, G. (2024). A systematic review and meta‑analysis on early‑childhood‑caries global data. BMC Oral Health, 24(1), 835.
Make an appointment for consultation today.
Tokyo International Dental Clinic Roppongi
- Address: 5-13-25-2nd Floor, Roppongi, Minato-ku, Tokyo
- Phone: 03-5544-8544
- Closest Stations:
- Azabu Juban (Toei Oedo Line take exit7)
- https://youtu.be/iIeG91YEJTA The way to the clinic from Ohedo Line Exit7
- Azabu Juban (Tokyo Metro Namboku Line exit 5a )
- https://youtu.be/3yniFSfucGg The way to the clinic from Namboku Line Exit 5a
- Roppongi (Hibiya Line exit 3)
We look forward to helping you achieve a healthy, beautiful smile!